This month I would like to talk about an injury that presents itself over the winter months as the rugby season gets into full swing and as the six nations is upon us I would like to talk about SLAP lesions.
The glenoid labrum is a fibrocartilagenous structure that runs around the rim of the shoulder joint. It provides the first layer of stability to the joint to help prevent subluxation or dislocation. The top part of the cartilage provides the attachment point for the long head of biceps and glenohumeral ligaments.
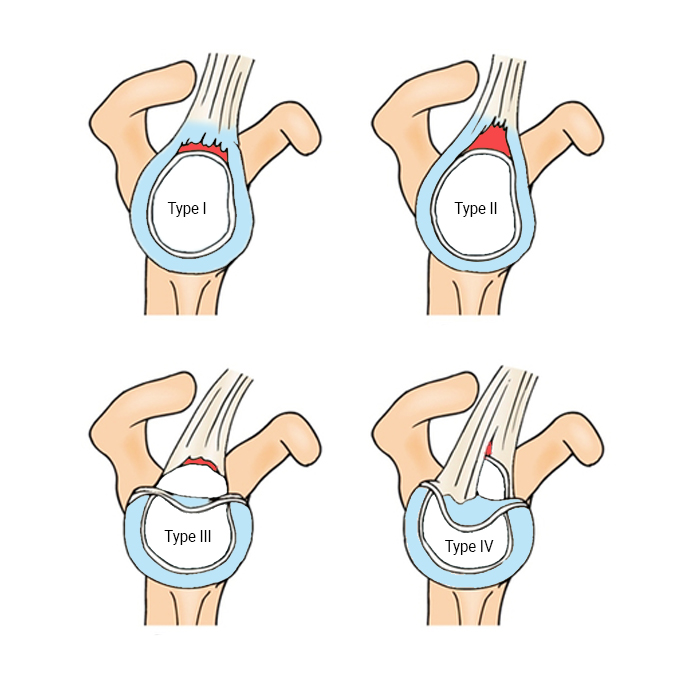
SLAP stands for superior, labral tear anterior to posterior and can be split into 4 categories.
Type 1 degenerative: This type has slight fraying of the cartilage but the long head of bicep attachment is intact and is most common in the middle age category.
Type 2: This type also has fraying but the glenoid labrum has slight detached from the bone as well as the long head of biceps.
Type 3: This type is like a meniscal tear where the tear is liek a bucket handle shape but the long head of biceps is still intact.
Type 4: This type is like type 3 but with an additional displacement of the long head of biceps.
The injury can occur with repetitive overhead loaded exercises of throwing motions that include external rotation such as in cricket and American football. It can also occur with direct hits to the shoulder such as rugby tackling or falling onto an outstretched arm.
Studies have shown that SLAP tears due to degenerative changes increase is we hit middle age and people between the age of 51-65 are twice as likely to get a tear when compared to people between the age of 30-35.
Sign and Symptoms
- Pain in the front of the shoulder.
- Pain from repetitive throwing
- Popping, catching and grinding.
- Clicking into the joint on overhead motions such as in a tennis serve or pull ups.
- The client has had a previous rotator cuff pathology which has lead to a tear later down the line.
Test and treatment
Certain shoulder test can be performed to help is rule in/out a SLAP tear. Depending on the level of tear, we will use those tests in clinic to guide our treatment plan. MRIs can be useful to help with the type if tear
Type 1 and 3 tears can respond well to non operative treatment protocols with rehabilitation centered around strengthening and loading the functional impairments and improving flexibility to the joints that have decreased range of motion.
Type 2 and 4 tears tend to need an orthopedic consultants analysis and if surgical intervention is indicated they are followed up with the same rehab principles stated above.
So if you have being showing any of these signs or symptoms please do get in contact so we can helps guide you with the best path for treatment.
Till next time
Mario
Leave a Reply